
By Mayank Kedia, Research Associate (Technology Solutions) – ICTPH, and A.R. Selva Swetha, Research Analyst – ICTPH
With the Health Systems approach we are aiming to take, which comprises preventive screening, curative, and community and clinic-based intervention components, we at ICTPH recognise how invaluable population-based screening is. We have been grappling with the issue of population-based screening for a while now, our journey beginning with the OMR-based PISP. This was a comprehensive, age-bracket specific individual risk profiling protocol, based on international screening guidelines, and administered in the field by trained Community Health Workers. But along the way, the numerous latencies involved in the process, compelled us to look for a more efficient solution. (For more on this, see Deepak’s blogpost) Hence was born the Rapid Risk Assessment (RRA), a short 15-minute questionnaire that will be administered on Android mobile phones to all the adults in the catchment area of 10,000 individuals around each of our Rural Micro Health Centres (RMHCs). The World Health Organization (WHO) defines screening as the “presumptive identification of unrecognized disease or defects by means of tests, examinations or other procedures that can be applied rapidly”. And it is this rapidness that the RRA aims to bring, with its short set of questions which are of immediate actionable impact.
The Rapid Risk Assessment Questionnaire:
- Marital Status
- Pregnancy
- Blood Pressure
- Anthropometric Measures: Weight, Height, Waist and Hip Circumferences
- Personal History – Diabetes and Hypertension
- Tobacco Consumption (chewing or smoking)
- Women’s Health – Inter-menstrual bleeding and post-coital bleeding in the last 3 months
The objective of the RRA is to risk-profile the community and identify sub-populations as target groups for our interventions. The final questionnaire itself was the result of two months of deliberation, where the rationale for each of the questions was carefully researched and debated upon. As researchers, we understood the significance of the one-time opportunity to elicit information from each individual in our catchment, but in keeping with the principle of the RRA knew it would have to be directly actionable, without compromising on the rapid nature of the exercise.
Logic was built into the survey so that one is asked only questions that are applicable – for example, male respondents, and unmarried respondents were excluded from the pregnancy question. The instant risk-profiling capability of the RRA means that at the end of the survey, based on the responses, the surveyor is prompted a next action on the phone – e.g., if the respondent is pregnant and has had a history of high BP, the respondent may be at risk for pre-eclampsia, and a prompt appears on the phone for the surveyor to dispense the appropriate advice and prompt her to seek care. Similarly, a person at risk for cardiovascular disease, is prompted to be given a Heart Health voucher which entitles him to a visit to the RMHC for free diagnostic testing and medication, if required.

Heart Health Voucher |
Vision Voucher |

Infant Voucher |
A respondent is issued a Heart Health Voucher in any of the following cases:
- Is positive on at least 2 risk factors (Age, BMI, Waist-Hip Ratio, Tobacco Consumption)
- High Blood Pressure
- Positive Personal History of Diabetes/Hypertension
All those above 45, at risk for Presbyopia, are given a Vision Voucher for an eye screening at the RMHC
All infants enrolled from 6-24 months are issued Infant Cards which would entitle them to nutritional assessments at the RMHC.
The technology platform used was Commcare and its related back-end solution Commcare HQ, solutions from Dimagi (See blog detailing the ICTPH partnership with Commcare). The mobile phone selected for this exercise was the Samsung Galaxy Pop running Android v2.1 OS, with GPRS connection enabled.
Current project
Our first pilot with the RRA is in the catchment area around our RMHC in Karambayam. Our catchment area in Karambayam consists of approximately 2200 households and about 7,000 adults. In the case of Karambayam, the Enrolment exercise capturing the demographic details of all individuals in the catchment area, and issuing each household with a unique ID, had not been done earlier, and so the RRA is being carried out concurrent to the Enrolment. In Karambayam, we have also been piloting a network of Community Health Workers (termed Guides within our system), and they have been deployed in administering the RRA in the field. In replicating the RRA in other geographies, however, Survey Officers locally hired on a contractual basis will carry out the task.
In going about planning the whole exercise there were a number of things to consider. Our very first draft plan looked like this:
- Use census data to identify the catchment area
- Map the whole area using mytracks
- Divide the area ito sub-divisions
- Finalise RRA questionnaire
- Rapid risk form needs to be created/tested on Commcare ODK
- Create back-end technology platform
- Revisit area allocation for guides to account for drop outs
- Create the bar-coded ID cards
- Design and print the various bar-coded intervention cards
- Communication material to be distributed at the household
- Procuring of phones/SIM cards
- Planning of beats with approximate population figures for each subdivided area – to be taken up after mapping exercise and census data collection
- Field trial with 2 Health Extension Workers/ Nurses /Field Supervisors
- Training of the Guides
- Launch
The run-up to the launch saw a flurry of activity: from long nights at the printer’s getting the front-back alignment of the bar-coded vouchers right to planning the day-by-day training schedule for the Guides, we were constantly kept on our toes. The Guides underwent six days of training, beginning with the basic use of the mobile phone, understanding the concepts of Enrolment and RRA, the meaning of the transliterated questionnaires, before moving on the phone application itself. The exciting part was gaining insights from the training on a daily basis and being able to incorporate our learning real-time. From tweaking the wording of the questionnaire based on the Guides feedback in order to elicit accurate responses, to identifying common errors on the field and building appropriate checks in the form, to changing the ordering of the options in the multiple-choice questions in order to optimise Guide time, to adapting the training to address the Guides’ weaknesses, what made the it all enjoyable was iterating and improving upon things as a result of that daily connect to the field.
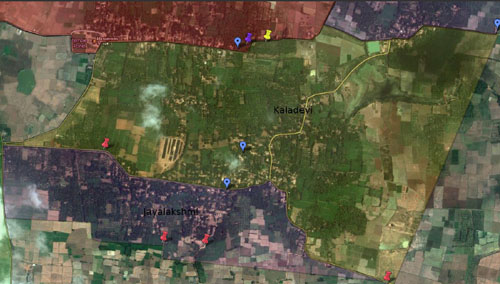
Each Guide was given a map of their allocated area. In allocation, as far as possible, natural boundaries were used as demarcators, in order to ensure that none of the houses end up being visited twice.

The Guides with the Android phones and Training manuals during the training

Our Guide Jayalakshmi explains to the class the filling of the Enrolment form, as Alex, the Field Supervisor looks on

Uma administering the RRA at a household
A two-day pilot in the field helped in understanding challenges in the field, in determining the performance benchmarks for the Guides, and in setting the forms per day threshold, given we are implementing a pay-for-performance incentive structure with two differential pay buckets. We rolled-out the Enrolment-cum-RRA on September 26th, and three and a half weeks into the project, the numbers currently stand at 840 households enrolled and 1490 RRAs completed.
It will be a very exciting next few weeks as we see how things pan out on the field. Watch this space for an account of our experiences from the field and also documentation of the whole exercise in greater detail in our upcoming paper.

Leave a Reply
1 Comment on "The launch of mobile phone-based rapid risk-profiling of our populations"
[…] through Sprinkles: A Case Study | The ICTPH Blog on Launch of Sprinkles Nutrition InterventionThe launch of mobile phone-based rapid risk-profiling of our populations | The ICTPH Blog on Partnership with Dimagi: Use of CommCare to carry out Rapid Risk Assessment through Health […]