
By Rosemary Stafford
The Sugha Vazhvu Guide program, initiated in August 2010, is a critical component of ICTPH’s Rural Micro Health Centre (RMHC) approach to primary care delivery.
Given its mission to build a primary healthcare system throughout remote and rural communities in India, ICTPH senior management was keen to find a scalable method of service delivery that would connect the physician at the RMHC with the community members in the surrounding catchment. As you may have read about in previous posts, the Sugha Vazhvu Guide program was designed to do just that. In its first year of operation, each Guide was responsible for the health of approximately 200 households, administering the Population based Individual Screening Protocol (PISP), conducting follow-up visits, providing clinical assistance, and supporting intervention implementation in her locality.
Purpose of Evaluation
As program designers and implementers well know, evaluation is key to any program’s success and eventual expansion. Knowing this, ICTPH made it a priority after the Guide program’s first year to assess how the program was functioning and if it was in fact bridging the RMHC to the community. ICTPH had already identified fundamental challenges with the existing Guide model, making it a nonviable scalable CHW model to use in future RMHCs. To address these issues and explore alternative solutions, ICTPH hired me, an external professional, to conduct a systematic process evaluation of the Guide program.
As requested by ICTPH management, the purpose of the evaluation was fourfold:
- To take stock of the program’s activities and outputs in the first year,
- To clarify the goals and outcomes of the Guide program moving forward, and
- To identify program activities and structure that need to be modified in order to accomplish the desired program outcomes
- To propose a scalable restructured program that incorporates lessons learned from the first year and best practices in the field of community health
Evaluator’s Background:
Before coming to Thanjavur, I completed my graduate studies at Washington University in St. Louis with a Master in Social Work and a focus in health research. A significant component of my graduate studies involved training and practice in program planning and evaluation. In Spring 2011, I conducted an evaluation of another community health worker program, the Community Referral Program administered by the St. Louis Integrated Health Network. My graduate studies and firsthand evaluation experience aligned with the skill set necessary for the Guide evaluation, and I was recruited by ICTPH to conduct a process evaluation of the Guide program in Karambayam.
Since joining in July 2011, I have completed the evaluation and assisted ICTPH with restructuring the Guide program to incorporate lessons learned and best practices in the field of community health. Today I will share one key component of the final report: the program logic models.
A commonly used tool among program planners, implementers, and evaluators, logic models help to define the given program’s goals and then depict how the program’s activities are intended to accomplish the stated goals. Logic models visually articulate a “series of ‘if-then’ relationships that, if implemented as intended, lead to the desired outcomes.” (University of Wisconsin-Extension, 2010).
Below you will see two logic models:
Guide Program Year 1
The first model depicts the Guide program structure and function from August 1, 2010-August 31, 2011. This model was dated before it was created. However, it serves as a point of comparison for stakeholders, outlining from where the program originated. It also functions as a evaluation tool, providing as a starting point from which the evaluator can determine how (and why) the program implementation departed from the program plan.

Guide Program Year 2
The second model depicts the restructured Guide program, as defined by new contract terms initiated on September 1, 2011. This model incorporates literature on best practices in community health worker programs, lessons learned from year 1 of operations (based on staff and Guide interviews), and new activities as necessitated by ICTPH and Sugha Vazhvu’s organizational needs (Rapid Risk Enrolment, high-risk patient follow up, etc.).
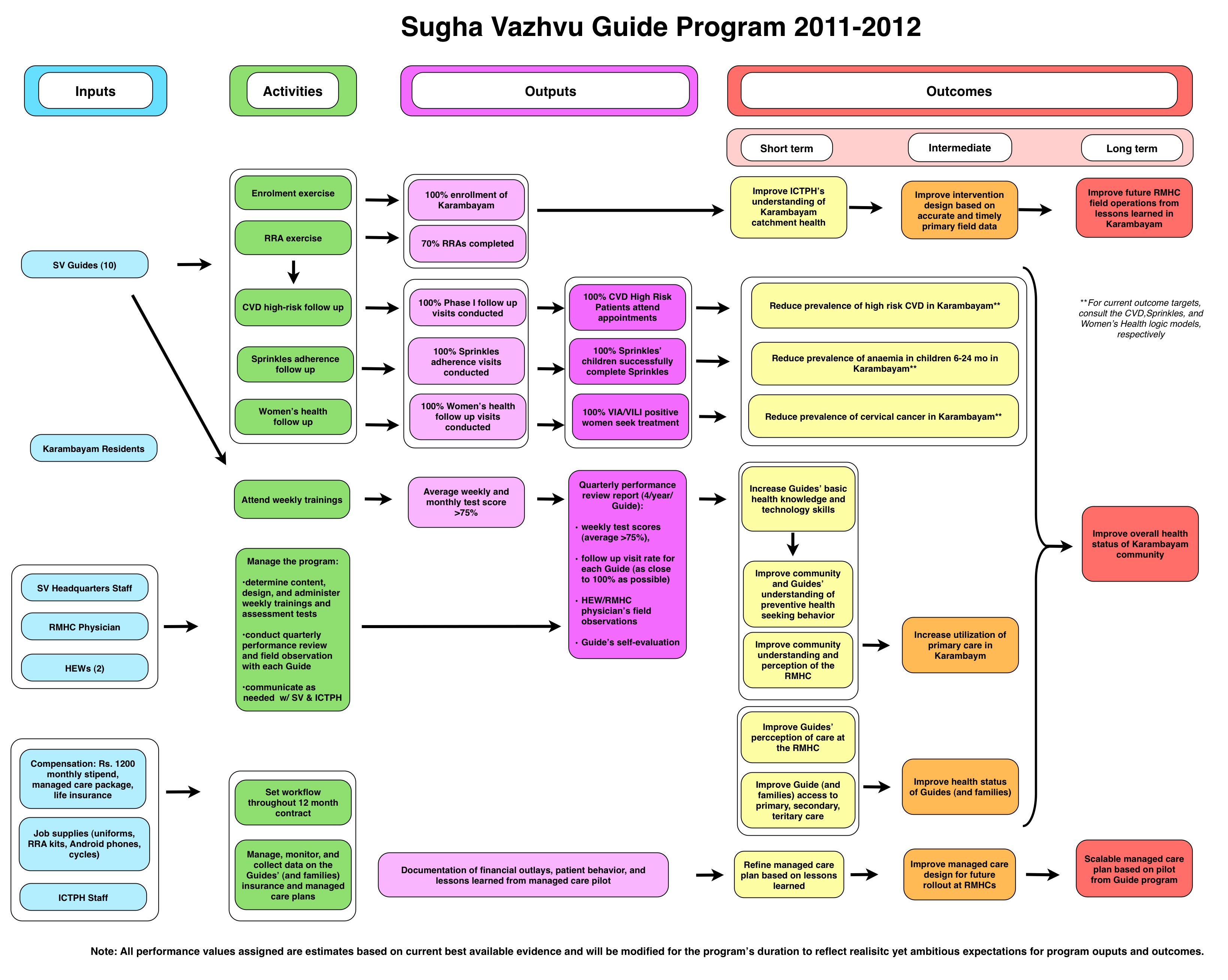
ICTPH staff will regularly refer to the Year 2 model throughout the program’s duration to:
- Monitor if output targets are being met,
- Revise program activities as necessary, and
- Ensure the Guide program is operating in the manner necessary to meet program goals.
Outcome of Evaluation
The Year 1 Guide Program Evaluation is finished, and it was a tremendous success. The evaluation helped ICTPH to clarify its goals for the program and to restructure the Guide model in order to achieve these objectives. When the evaluation began, it was unclear if the program would continue in its second year, and it was uncertain who among the 12 Guides would choose to renew her contract if offered. As a result of the systematic, evidence-driven evaluation, ICTPH invested in the program for a second year. And, 100% of the Guides stayed with the program in its second year. The final report will be posted here next week. Stay tuned for more detailed results.

Leave a Reply
1 Comment on "Karambayam Guide Program – The previous year and the year ahead the Logic Model Approach"
[…] enthusiasm, and a plan. You can read a bit more about why I was conducting the evaluation in this previous post. But, in short, ICTPH’s Community Health Worker (CHW) model, the Sugha Vazhvu Guide program, […]